Female 41. years old presents to regional hospital Leskovac with chest pain that started 30 minutes ago with unprovoked, severe chest pain that propagated to the left arm a lower jaw and was accompanied by headache.
STEMI diagnosis was confirmed, and she was loaded with Aspirin and Clopidogrel and transported to the PCI center (KBC Niš). The patient complained of elevated blood pressure during her menstrual cycle which was accompanied by headaches.
Risk factors for CVD: arterial hypertension, obesity (BMI >40)
ECG on admission:
 LAB: TnI 2.180; K 3.1; Hol 4.47; LDL 2.49; HDL 1.24; TRIG 1.6
LAB: TnI 2.180; K 3.1; Hol 4.47; LDL 2.49; HDL 1.24; TRIG 1.6
In CICU she received LMWH (Clexane 100mg c.s) and was sent to the cath lab.
Angiography showed moderate lumen narrowing in mid-LAD with TIMI3 flow.
Angiogram SCAD; classified as normal (without significant lesions)
After returning from a cath lab, the patient is asymptomatic.
During her stay in CICU she was on DAPT an LMWH (Clexane 100mg BID).
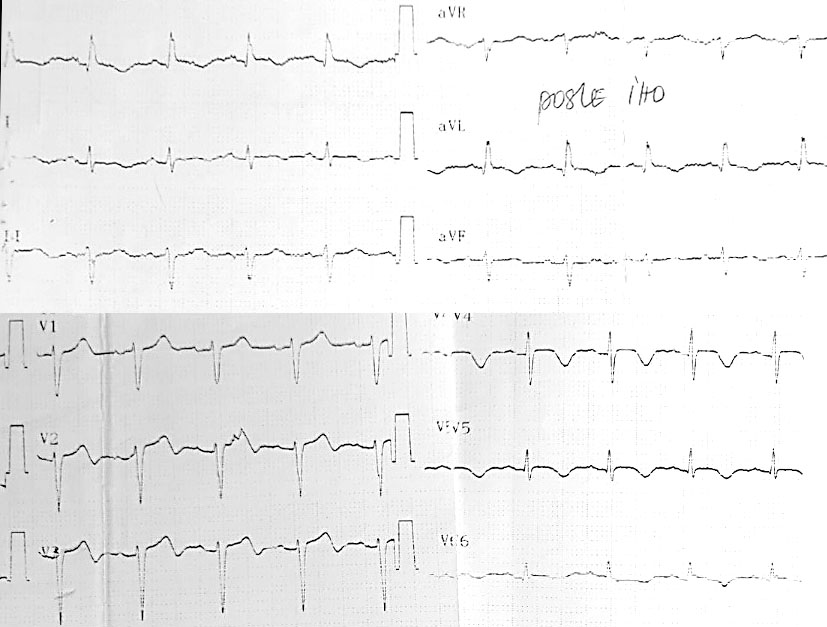
ECG after cath lab:
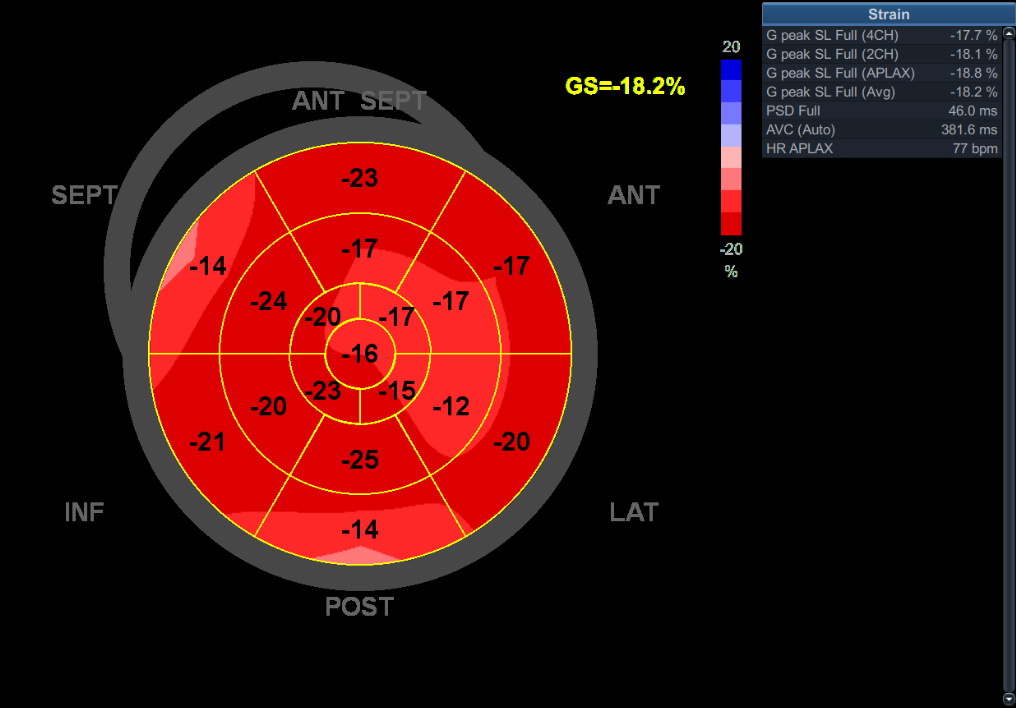
 ECHO day one:
ECHO day one:
After a hearth team discussion and angiography review, SCAD was suspected.
On the fourth-day control angiography an OCT were performed confirming SCAT type 2 with intramural hematoma and no flap i mid-LAD.
LMWH was discontinued.
Patient discharged with 1 month DAPT and the Clopidogrel 75mg permanently.
ECG on discharge:

Coronary angiograpy after one month:
ECHO after one month:
1. Do you think that first angiographic results are misinterpreted often?
2. Would you do an OCT in the acute phase on a patient like this?
3. Since the patient didn’t undergo a PCI would you give DAPT up to one month?
4. Should a patient like this be sent to cardiac rehabilitation?