A 37-year-old female presented with a concerning episode of chest pain that radiated to her left arm, lasting approximately 10 minutes.
Notably, she has no known chronic diseases and does not possess any risk factors for cardiovascular disease.
Upon admission, her troponin level was measured at 2.27 ng/ml, prompting her admission to the Intensive Care Unit (ICU) for further evaluation and management.
ECG at admission:

An elective coronary angiography was done on the seventh day following her admission.
Coronary angiography:
RCA with 99% stenosis i medial segment and 80% in medio-distal segment.
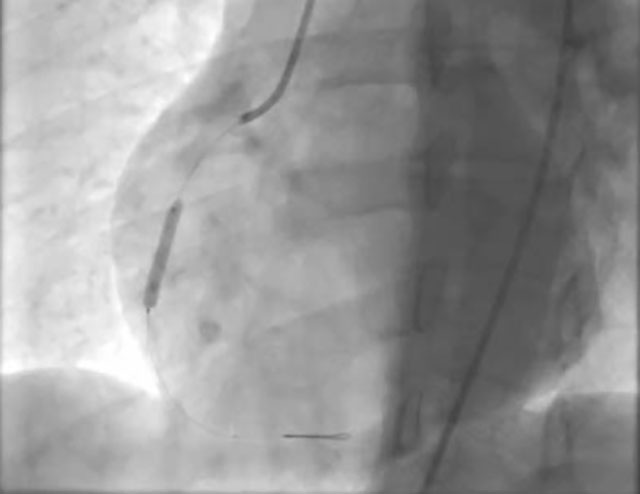
PCI was preformed:

ECHO showed LV 4.72/3.28, EF:57%, hypokinesia of inferior wall.
One year later, a woman, 39 years old, presents with acute coronary syndrome (ACS), without risk factors for coronary heart disease (CHD), and without comorbidities.
She is the sister of a previous patient!
She is experiencing chest pain accompanied by nausea and vomiting. Symptoms started one day prior to admission. The pain is located behind the sternum and radiates to both arms down to the elbows.
Her troponin levels was measured at 0,00… 1,84… 12,55… 0,10 ng/ml
ECG at admission:
 ECG during chest pain:
ECG during chest pain:

The patient was on medical therapy for 3 days, and subsequently, a coronary angiography was performed. In the meantime, there were multiple episodes of chest pain that responded to sublingual nitroglycerin (NTG) or NTG infusions.
Coronary angiography:
In the medial segment of LAD, there is SCAD type II with TIMI flow I-II.
It has been decided to continue with medical therapy.
Th: ASA 100mg, Clopidogrel 75mg, Nebivolol 5mg, Atorvastatin 60mg, PPI, NTG prn.
ECHO showed LV:5.15/3.22, EF:55% hypokinesia of apex and distal half of lateral wall
Coronary angiography after 3 months shows complete recovery:
Author: Prim Dr sc med Vladimir Mitov, FACC, KC Zaječar
Did the first sister had SCAD?
Would you treat the first sister conservatively if you had this knowledge about SCAD?