A 37-year-old female presented with a concerning episode of chest pain that radiated to her left arm, lasting approximately 10 minutes.
Notably, she has no known chronic diseases and does not possess any risk factors for cardiovascular disease.
Upon admission, her troponin level was measured at 2.27 ng/ml, prompting her admission to the Intensive Care Unit (ICU) for further evaluation and management.
ECG at admission:

An elective coronary angiography was done on the seventh day following her admission.
Coronary angiography:
RCA with 99% stenosis i medial segment and 80% in medio-distal segment.
PCI was preformed:
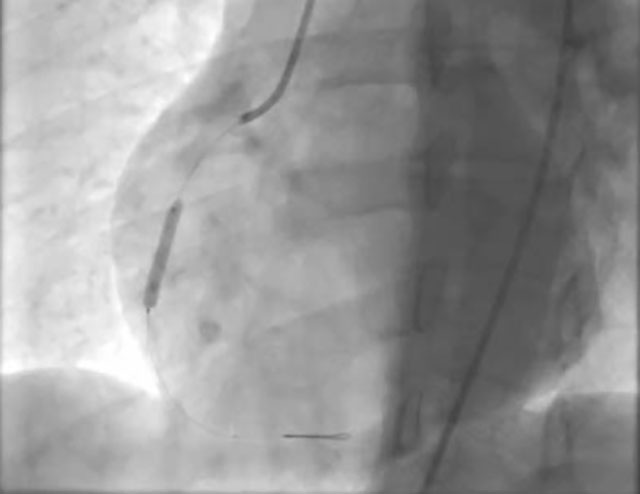

ECHO showed LV 4.72/3.28, EF:57%, hypokinesia of inferior wall.
One year later, a woman, 39 years old, presents with acute coronary syndrome (ACS), without risk factors for coronary heart disease (CHD), and without comorbidities.
She is the sister of a previous patient!
She is experiencing chest pain accompanied by nausea and vomiting. Symptoms started one day prior to admission. The pain is located behind the sternum and radiates to both arms down to the elbows.
Her troponin levels was measured at 0,00… 1,84… 12,55… 0,10 ng/ml
ECG at admission:
 ECG during chest pain:
ECG during chest pain:

The patient was on medical therapy for 3 days, and subsequently, a coronary angiography was performed. In the meantime, there were multiple episodes of chest pain that responded to sublingual nitroglycerin (NTG) or NTG infusions.
Coronary angiography:
In the medial segment of LAD, there is SCAD type II with TIMI flow I-II.
It has been decided to continue with medical therapy.
Th: ASA 100mg, Clopidogrel 75mg, Nebivolol 5mg, Atorvastatin 60mg, PPI, NTG prn.
ECHO showed LV:5.15/3.22, EF:55% hypokinesia of apex and distal half of lateral wall
Coronary angiography after 3 months shows complete recovery:
Author: Prim Dr sc med Vladimir Mitov, FACC, KC Zaječar
Did the first sister had SCAD?
Would you treat the first sister conservatively if you had this knowledge about SCAD?
Very difficult question. It means excellent question.
Pobably I would live it as it is… if I had an information on her sister’s disease … than close in-hospital monitoring and new coronary angio before discharge or in case of symptom reappearance.
There is also a possibility of catheter induced dissection (as an add on preexisted SCAD… I would call it as “hybrid” vessel injury = SCAD + catheter induced dissection). Catheter was in a very deep position aiming to the vessel wall. And we have witnessed some cases as I mentioned. Patient should be screened for every possible elastopathy cause.
I am happy and honored that an interventional cardiologist like Siniša joined us in analyzing SCAD cases!
Thank you colleagues from Zaječar for sharing these two cases with us!
I would certainly treat the first patient as SCAD, even if I didn’t know that she had a sister with SCAD: age, sex, risk factors, smooth edges of the lesion…that the dissection spreads after stent implantation in ACDx is evidence of SCADA.
I think it is good to say about SCAD: FIRST BELIEVE IT IS SCAD, IF NEEDED JUST FOLLOW, IF IT GETS WORSE THINK ABOUT IMAGING METHODS AND CUTTING BALLOON, IF NECESSARY IMPLANT A STENT
Good cases! I also think in first case that is possible combination of SCAD and iatrogenic coronary artery dissection in proximal part of RCA. But in that time (2014, no intracoronary imaging in all centers in Serbia) I would performed PCI at index procedure. Both sister should be tested for FMD and connective tissue disease.
Dear Prof Apostolović, thank you for opportunity to present our cases. This two cases is “zero” or “index” patients in our professional carriers to start study problem with SCAD. Prof Stojković and Prof Petrović, thank you for comment’s! For long time we believed that in first patient after implantation 1. stent on lesion we had new dissections below and above from stent in same time. Idea about artificial dissection with guiding catheter “hybrid” vessel injury = SCAD + catheter induced dissection probably is the real situation.
Dear colleagues, thank you for presenting such interesting cases. As prof. Petrović said, ten years ago the imaging was available in few PCI centers in our country, so the thypical SCAD image of LAD, occured in second sister, with age, sex, etc. helped a lot. I am very glad that the Cath Lab of the hospital in Zaječar started IVUS in this year, which will help in further diagnostics and work. Maybe also in similar cases in the future. Congratulations to doctor Mitov for excellent solutions and speaking about SCAD, which is in my opinion the most important.
Another intersting and very useful presentation of SCAD in the means of advancing our knowledge on this important topic. Even on DAPT, sister developed complete healing of LAD which is very interesting for me, underlying our ongoing dilemmas on what is the best treatment approach. Many thanks to prof Apostolovic on this initiative and all the colleagues, and my teachers, sharing their cases and thoughts.
Thank you for comment, this cases are excellent show developing therapy SCAD patient during time. In 2014. and 2015. it was impossible discharge patient with any form of CAD without DAPT, now situation is completely different!
Great case(s) from colleagues! And patients are treated accordingly, especially in the second “sister” case.
SCAD runs in families. It has to be acknowledged and emphasized!
Many patients who have experienced SCAD report a family history of early, unexpected, or peripartum death or premature cardiovascular events occurring in young or low-risk relatives. Family history may facilitate better risk stratification and accurate diagnosis of myocardial infarction or sudden death of unclear etiology in the families of patients with SCAD, and may also help health professionals recognize the risk of SCAD in young women with symptoms suggestive of ACS or the need for prompt attention in risk relatives. This may include high-definition imaging or genetic testing. Computed tomographic angiography or magnetic resonance angiography should be used to screen the brain, neck, and visceral arteries because extra coronary vasculopathy, such as fibromuscular dysplasia, aneurysms, and dissections, are common in individuals with SCAD. This is crucial for patients who have extra coronary vascular disease symptoms or signs, a diagnosis of fibromuscular dysplasia, and a family history of aneurysms, dissections, or sudden, unexpected death. SCAD patients may potentially benefit from formal medical genetic investigations and familial genetic paneling towards genetic connective tissue diseases. Since there is no medical preventive strategy, the patient’s relatives at risk (namely female gender close relatives) are encouraged to pursue moderate daily aerobic activity and resistance training with low weight and more repetitions because extreme physical activity has been linked to SCAD. Patients are advised to avoid weight lifting, bodybuilding, competitive racing, or athletic pursuits at high-intensity levels.
Dear Zlatko,
Thank you for comment and very detailed explanation pathophysiology of SCAD!
Dear all,
I am sending a new metanalyses of genetic insights into spontaneous coronary artery dissection. It is precisely the topic of recognizing predisposition, and therefore prevention, about which Zlatko spoke.
Nature Genetics volume 55, pages 912–913 (2023)
Genetic and biological insights into spontaneous coronary artery dissection
Meta-analysis of genome-wide association studies of spontaneous coronary artery dissection (SCAD), an important cause of myocardial infarction, identified 11 risk loci that involve genes related to artery integrity and tissue-mediated coagulation. Evidence supports SCAD as a genetically distinct condition from atherosclerotic coronary artery disease.
Tissue coagulation as a novel mechanism in SCAD
. Integrative functional annotations
prioritized genes that are likely to be regulated in vascular smooth muscle
cells and artery fibroblasts and implicated in extracellular matrix biology.
One locus containing the tissue factor gene F3, which is involved in blood
coagulation cascade initiation, appears to be specific for SCAD risk. Several
associated variants have diametrically opposite associations with CAD,
suggesting that shared biological processes contribute to both diseases,
but through different mechanisms. We also infer a causal role for high blood
pressure in SCAD. Our findings provide novel pathophysiological insights
involving arterial integrity and tissue-mediated coagulation in SCAD and set
the stage for future specific therapeutics and preventions