A 57 years-old female was admitted in regional hospital because of NSTEMI with OHCA due to the VF in October 2022.
Risk factors for cardiovascular diseases: hypertension, positive family history for CVD and smoker.
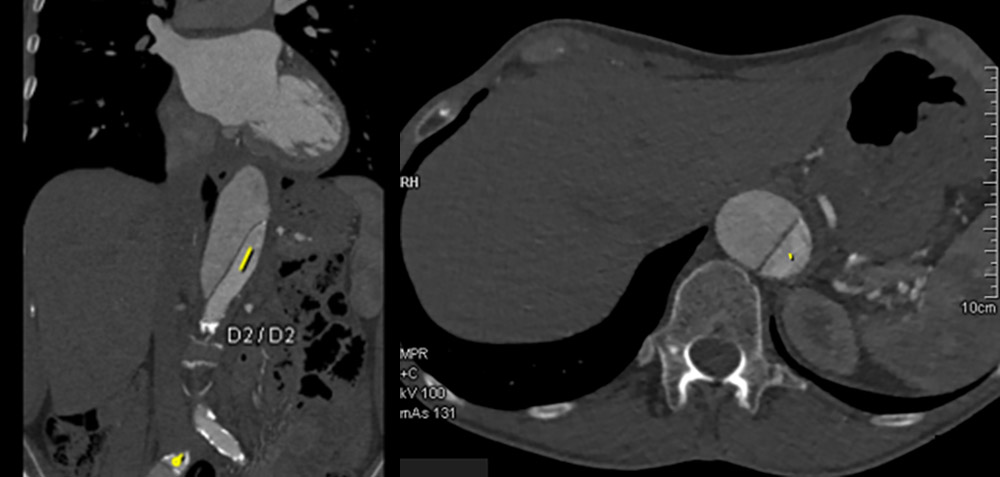
Three years ago Stanford B dissection was registered and conservatively treated.
 After initial stabilisation patient was transferred to the tertiary center for coronary angiography and further diagnostic.
After initial stabilisation patient was transferred to the tertiary center for coronary angiography and further diagnostic.
At the admission she was without any symptoms.
Status at the admission: alerted, oriented, hemodynamically and rhythmically stable, Killip I.
ECG on admission:

ECHO:
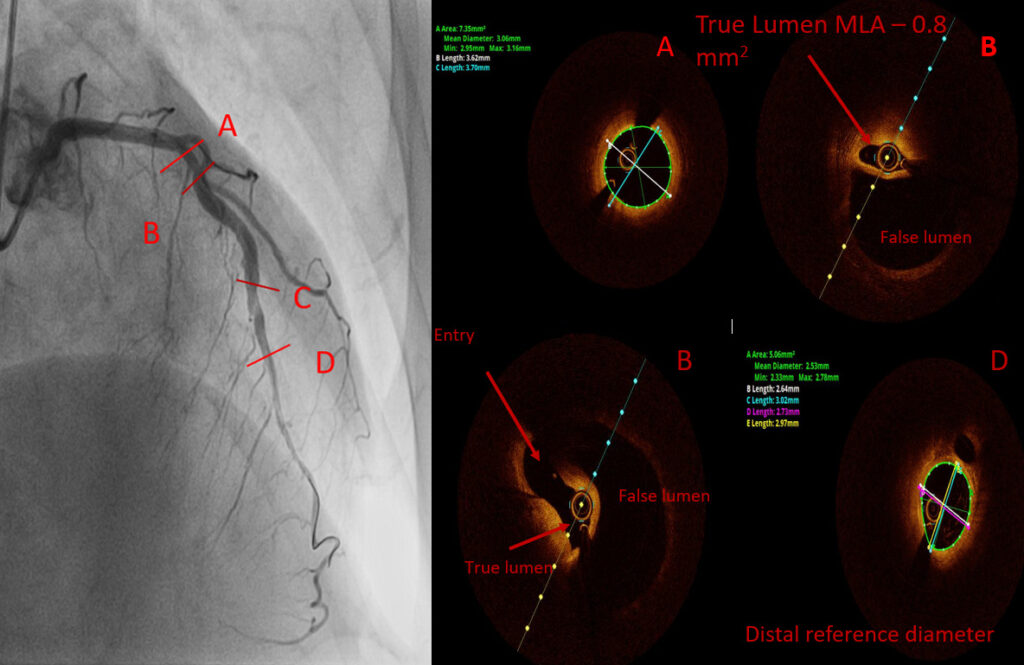
Coronary angiography:

Operators: Prof. Dr I. Ivanov, Doc. Dr M. Čanković, IKVBV Sremska Kamenica
Would you decide for PCI LAD?
Part two
In the second act was planned PCI LAD with intravascular imaging ( OCT).
During the hospitalization, the patient had symptoms of COVID-19 infection and was transferred to COVID hospital Novi Sad.
Two weeks later OCT guided PCI LAD was performed.
OCT pullback before PCI
PCI LAD

OCT pullback after stent implantation

Stent postdilatation

Final result:

Great images of the case! Since patient was without chest pain, with a TIMI 2-3 flow in LAD, would opt for conservative treatment (no PCI, no DAPT or LMWH, control angio before dismission). Best regards for colleagues from IKVB Sremska Kamenica!
It is a really great case. I am not an interventional cardiologist, however, it is very illustrative. And what did you do? Could you inform us about the FU of this patient, please?
Thank you for these experience.
I would also stay to a conservative approach.
How do you explain the association of aortic dissection and SCAD?
What do you think about contrast retension before LM? Calcium?
Very interesting case. Of curse conservative approach is correct choice for this patients. Fibromuscular dysplasia can be pathophysiological mechanism who can explain aortic dissection and SCAD. Shadow (contrast retention) before LM is similar like calcium, but must think about aortic dissection especially in patients with history for aortic dissections and SCAD!
Since the patient had NSTEMI complicated with VF and OHCA I wouldn’t be brave enough to proceed with conservative treatment without a further diagnostic.
I would do intracoronary imaging to assess the distribution and MLA of the true lumen. If the true lumen is severely compromised I would proceed with PCI. I agree with Dr Mitov that FMD can be the cause.